This page has information on:
The first step to being able to spot any cancer symptoms is to know your body and what is normal for you.
You may or may not have been taught about the gynaecological organs (female reproductive system) at home or at school, but it is never too late to learn about your body, and how you can look after your health.
The reproductive system
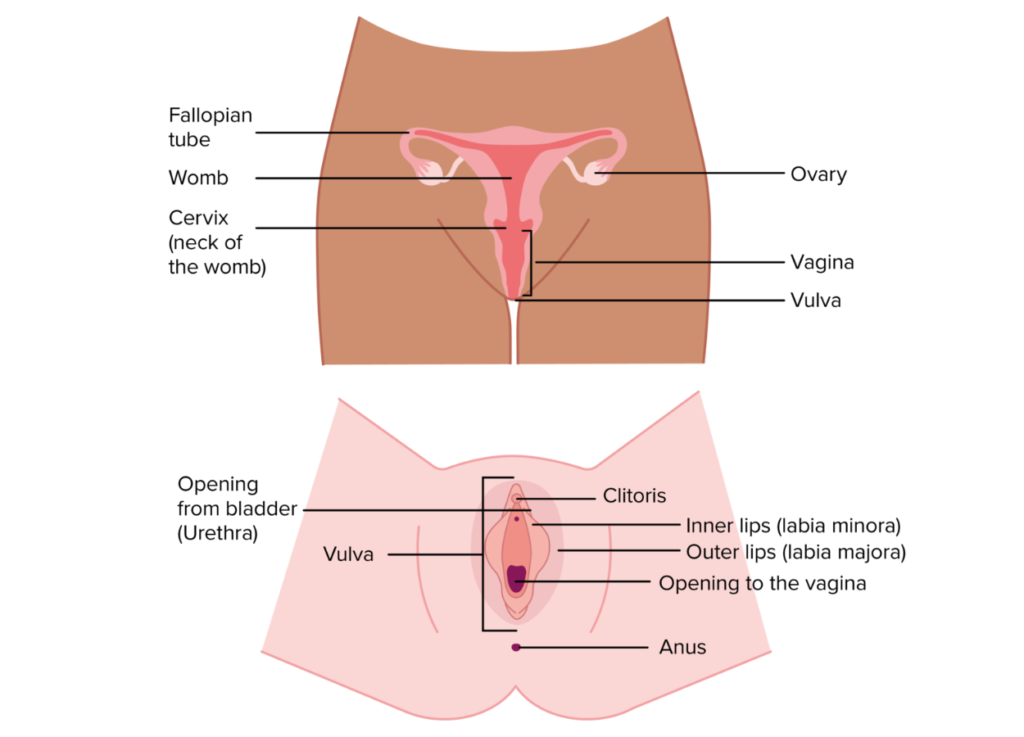
What is the cervix?
The cervix is the neck of the womb. It connects the bottom of the womb to the vagina. It is the shape of a doughnut. The cervix is where a sample is taken from during your cervical screening tests.
What is cervical cancer?
Cancer of the cervix can affect anyone with a cervix at any age. It is most common between the ages of 30-34. It is very rare under 25 years of age. In the UK we have a very successful cervical screening programme. It saves over 5,000 lives each year. Anyone with a cervix can get cervical cancer, including trans men and non-binary people with a cervix.
Key cervical cancer statistics
30-34
the age cervical cancer is most common
5000
lives a year are saved in the UK by cervical screening
3,250
number of people diagnosed each year in the UK
How does cervical cancer develop?
There are two main types of cervical cancer. The most common is squamous cell carcinoma. 8-9 in every 10 people with cervical cancer will have this type. The next common is adenocarcinoma.
Nearly all squamous cervical cancers are caused by human papillomavirus (HPV). HPV is a very common virus. 8 in 10 of us will come into contact with it in our lives. HPV is transmitted through skin-to-skin sexual contact. Most of the time our bodies will clear the virus and it won’t cause any issues. Rarely, HPV lingers and develops into cell changes or cancer.
There are more than 200 different types of HPV. Some are low-risk and don’t cause cancer. Others are high-risk and can cause cancer.
What are the symptoms of cervical cancer?
The symptoms of cervical cancer aren’t always obvious. The most common symptoms are vaginal bleeding that is new or different for you. This includes:
- Vaginal bleeding during or after sex – this is often the first sign
- Bleeding in-between periods
- Bleeding after the menopause, (12 months since your last period).
Other symptoms include:
- Lower back or pelvic pain
- Pain or discomfort during sex
- Changes to vaginal discharge like a change to smell.
If you have any of these symptoms, it is important that you see your GP, even if you have recently had a clear cervical screening test. It is more likely to be caused by something less serious than cancer, but it is always worth getting them checked. Just in case. The earlier cervical cancer is caught, the more treatment options there are and the best possible chance someone will have of successful treatment. Knowing what to look out for and getting any symptoms checked as soon as possible is really important.
What are the risk factors of cervical cancer?
HPV is the most common risk factor in cervical cancer, the others include:
- Age – Cervical cancer is more common in younger women and people with cervixes. 1 in 2 people under the age of 45
- Smoking – smokers are twice as likely to get cervical cancer. This is because smoking impacts the immune system and makes it less able to clear HPV
- Immunosuppression drugs – People who are on immunosuppression drugs long term (like people who have had an organ transplant), can be at a higher risk of cervical cancer as their immune systems are less able to clear HPV
- Other sexually transmitted diseases – People who may have another sexually transmitted disease, like chlamydia may be at a higher risk of cervical cancer
How is cervical cancer diagnosed?
Cervical screening tests are a test to help prevent cervical cancer, not diagnose it. The test looks for high-risk HPV, and if present, looks for changes to the cells which can be treated to prevent cervical cancer. If you have symptoms, your GP should refer you to a gynaecologist or colposcopy clinic for more tests.
Your gynaecologist or a nurse will look at your cervix with a small microscope with a light at the end, called a colposcope. They may take a small tissue sample called a biopsy, which will be sent off to a lab and looked at under a microscope.
Staging and grading cervical cancer
These tests will enable your doctors to find out if you have cervical cancer, which specific type of cervical cancer you have, and its stage and grade. All of this information will help your doctors work out the best treatment options for you.
The staging of cancer looks at how big the cancer is and whether it has spread.
The grading of cancer looks at the type of cancer cells you have and how they act, and whether they multiply quickly or slowly.
Cervical cancer stages:
- Stage 1 – early stage, where the cancer is only in the cervix
- Stage 2 – the cancer has grown into the top of the vagina or the tissues next to the cervix
- Stage 3 – the cancer has spread out of the cervix into the lower part of the vagina, pelvic wall, or lymph nodes
- Stage 4 – the cancer has spread to the bowel, bladder or other areas of the body outside the pelvis.
Cervical cancer grades:
- Grade 1 – slow growing, the cells look quite similar to ‘normal’ cells. This may also be called low grade or well differentiated
- Grade 2 – cells grow faster than grade 1. This may be called moderate grade or moderately differentiated
- Grade 3 – cells grow faster and are more likely to spread. This may be called high grade or poorly differentiated.
How can I help prevent cervical cancer?
HPV vaccination
All young people will be offered the HPV vaccine in year 8 as part of the school’s vaccination programme. The HPV vaccine has been shown to reduce the number of cervical cancers by 90%. The current vaccine covers nine strains of HPV: types 6, 11, 16, 18, 31, 33, 45, 52 and 58. There are five other strains of high-risk HPV, which can cause cancer, that are not yet in the vaccine. You can get the HPV vaccine from your GP up until the age of 25, or up to 45 if you are considered to be in a higher risk group.
Cervical screening
Cervical screening is a test to help prevent cervical cancer. It looks for high-risk HPV, and if it is present, cell changes. These cell changes aren’t cancer but could turn into cancer over time. If cell changes are found, they can be treated or monitored to stop them turning into cancer.
Removing cervical cell changes
If your screening results show that you have high-risk HPV and cell changes, you will be referred for a colposcopy which is a test to have a closer look at your cervix. This will check the level of cell changes and if you need any treatment.
Treatments for cervical cell changes
The most common treatments are:
- The cell changes are monitored to see if they return to normal on their own
- The cells are removed with local anaesthetic using a small wire with an electrical current running through it, called large loop excision of the transformation zone (LLETZ)
- The area with cervical cell changes is removed through surgery, usually under general anaesthetic. With cells taken off in the shape of a cone (called a cone biopsy).
More information and advice on prevention
We have lots more information and tips on preventing cervical cancer. You can also contact our Ask Eve nurses for free to chat about any worries or questions.
What are the treatments of cervical cancer?
If you are diagnosed with cervical cancer, your treatment will depend on the size and shape of the cancer.
Surgery
There are three main types of surgery for cervical cancer:
Trachelectomy
- Simple trachelectomy – removal of the cervix.
- Radical trachelectomy – the cervix, tissue around the womb (parametrium) and the top part of the vagina are removed. The womb is left in place. This surgery is usually done if the cancer is at an early stage. They may remove some lymph nodes to send them off for testing. This is to check whether the cancer has started to spread.
Hysterectomy
- Simple Hysterectomy – sometimes called a total hysterectomy. The cervix, womb and fallopian tubes are removed. If possible, the ovaries are left to prevent early menopause.
- Radical hysterectomy – The cervix, womb, ovaries and fallopian tubes are removed, along with the supporting tissue at the side of the womb (the parametrium) and the top part of the vagina. You might also need to have the lymph nodes in your pelvis removed.
- A hysterectomy may be offered for stage 1 and early stage 2 cervical cancers
- Pelvic exenteration – a major operation which may be used in advanced cervical cancer. This surgery removes the cervix, womb, ovaries, fallopian tubes, bladder, urethra and rectum.
Chemoradiation
Chemoradiotherapy may be used as a treatment for cancers that are stage 1B2 up to a stage 4A. During this treatment, you’re given chemotherapy and radiotherapy together. This is to help lower the risk of the cancer coming back. The most common chemotherapy drug used if your cancer has not spread outside your pelvis is Cisplatin.
Radiotherapy
This uses high energy x-rays to destroy cervical cancer cells. It can be given from outside (external) or inside the body (brachytherapy). External radiotherapy for cervical cancer may be followed by brachytherapy.
Brachytherapy
This is a type of radiotherapy which is delivered internally through the vagina. It gives a high dose of radiotherapy directly to the cervix. It may be given to reduce the risk of the cancer coming back or if you have locally advanced cancer that is difficult to treat with surgery.
The radiotherapy is planned by a team which includes a clinical oncologist, radiographers and physicists (specialists in radiation). Radiotherapy is planned for each patient and the amount of treatments needed (called fractions), may vary. Your clinical team will talk you through your treatment and answer any of your questions.
Life with/after cervical cancer
Living with and beyond cervical cancer can affect many areas of your life. Every woman is different, some may have lots of different emotions. You may also have effects from treatment months or even years later. Some women also come across stigma from the myths around HPV and cervical cancer. Getting cancer is never anyone’s fault. HPV is very common and anyone can get it. It is important that you get the help, support and information you need. You can contact our Ask Eve nurses to chat about any worries or questions.
More information and advice
We have lots more information and tips on gynae cancers. You can also speak to our Ask Eve nurses for free to chat about any worries or questions.

Our health information meets PIF TICK quality mark.
The PIF TICK is a seal of approval from the Patient Information Forum. It helps you know if health information is trusted, evidence-based and accessible.
To be PIF TICK approved, health information creators must prove they meet 10 key criteria and undergo a robust, independent annual assessment.
Information updated: April 2026. Next review due: November 2027
Real stories

Emma’s story
Emma joined us at the “Reception to celebrate Scotland’s progress towards eliminating cervical cancer”. She shared her story of her cervical cancer diagnosis and advocacy work.

V’s story
V was diagnosed with a rarer form of cervical cancer. She shares her story to help raise awareness.

Emma’s story
Emma writes about her cervical cancer diagnosis and treatment as she reflects on her journey.

Mandy’s story
Mandy reflects on her cervical cancer diagnosis and treatment nine years ago.